Book “Apallic syndrome”
Hemodynamic and neurorehabilitation features at apallic syndrome
Long-existing total disturbance of functions of the brain cortex is in the basis of the apallic syndrome (AS).

AS cases are mentioned in medical literature from the end of XIX century.
In 1940 Е. Kretschmer firstly used a term “apallic syndrome” and gave the first full description of its clinical picture.

„A patient is in prostration (immobile), he doesn’t sleep, his eyes are open. He either looks straight ahead or his eyes move aimlessly without focusing anywhere. Attempts to come into his notice are unsuccessful. Conversation with the patient, touching him or demonstration of objects don’t give any essential results. The reflex motions of alienation or defence are absent. In spite of non-sleeping, the patient can’t speak, recognize or follow social models of behavior, which he used to be taught before. According to neurological positions the described syndrome is characterized by the presence of panagnosia, panapraxia. Nevertheless, such elementary functions such as swallowing are present. And in spite of this, such primitive instincts as sucking and grasping appear.”


A term „vegetative state” was proposed by B.Jennet and F.Plum in 1972.
Apallic syndrome has to be:
- -dynamic
- -curable
- -regressive.


Vegetative state?

More often AS develops after serious brain injuries both of traumatic (car accident, gunshot wound etc.) and non-traumatic genesis (global cerebral ischemia as the result of heart arrest, respiratory standstill, asphyxia of various genesis, serious disturbances in cerebral circulation, infections of CNS, growth, endogenous and exogenous intoxication).
There are the following periods and stages in restoration of the nervous system when arousing from coma (Alexeyeva G.V., 1996):
Critical period (diencephalic-mesencephalic disorders predominate):
а)a stage of coma that is dangerous for life;
b) a stage of stabilization of vegetative functions.
Sub-critical period (except of symptoms of irritation, symptoms of fall appear and begin to dominate):
c) apallic syndrome;
d) akinetic mutism;
e) a stage of a verbal contact;
f) a stage of rough mental disorder;
g) a stage of patient’s rehabilitation as personality;
Distant period:
h) A stage of persistent residual phenomena or a stage of the complete restoration of functions of the nervous system.


„Resuscitation. Theory and praxis of resuscitation” М. Syha (1976) points out the theoretically substantiated confidence in rehabilitation up to the consciousness under explicit, relatively stable, functions of circulation, respiration and nervous system.


Estimations by data of etiological studies in countries of the Western Europe show 1-10.5 new cases only of traumatic AS per 100000 of population annually. According to data of some studies AS morbidity makes up 0,7–1,1 per 100000 of population, spreading – 2–10 per 100000 of population (Martynyuk V.Ju., 1998; International working party report on the vegetative state, 1996). .
Diagnostic signs
Diagnostic signs of AS in a certain patient are determined by a consultation of specialists based on certain signs, namely:
- -absence of awareness of himself and disability to interact with surroundings;
- -absence of proofs of any well-directed efforts and voluntary realization of behavioral reactions to visual, auditory, tactile and pain stimuli;
- -absence of proofs of speech comprehension;
- -preservation of varying but unordered circadian rhythm of unsleeping and sleeping;
- -sufficient preservation of autonomous hypothalamic and trunkal functions in order to live long with the help of symptomatic treatment and care;
- -disturbance of sphincters’ functions;
- -preservation of reflexes of cranial nerves (pupillary, oculocephalic, corneal, oculovestibular, spinal and deglutitory)
Typical opinions of research groups:
а) too slow progress on the background of the permanently existing subcompensation of functions of main systems in the organism;
b) unwarranted, to their point of view, material expenses, moral inputs both of medical staff and relatives of the patient.

Realization of active medical measures directed on restoration of hemodynamics enables to reduce a period of resuscitation, avoiding appearance of irreversible changes in the cerebral tissue, this increases the appearance of elements of minimal consciousness in the patient.
In USA a cost for treatment of such patients is 120 000 -140 000$ per year per one patient (Samborskyy J.V., 2001). Comparing economical expenses for treatment of one AS patient in USA in our country they reduce in 6-8 times with possible more positive results using new methods of the coordinated multidisciplinary approach (patented by the State Patent Office of Ukraine “Method of neurorehabilitation of patients with apallic syndrome № 72725 А on 31.12.03)

Our experience in neurorehabilitation AS patients enabled to single out 4 up-to-date methods of the coordinated multidisciplinary approach:
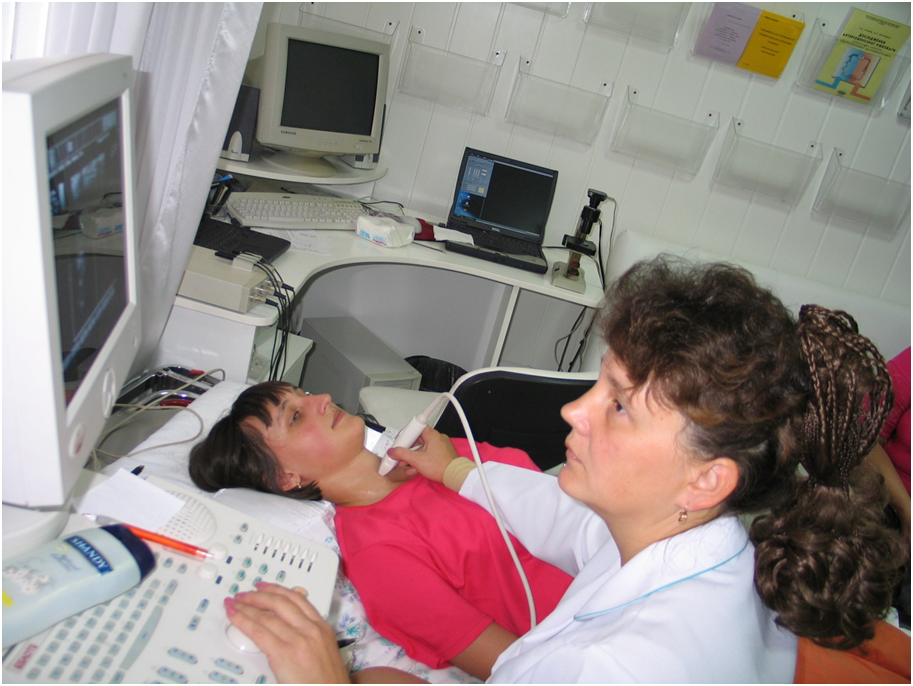
1. A thorough initial integrated minimally invasive observation of AS patient or in coma using USD of cerebral vessels, USD of the heart, USD of organs of the abdominal cavity and small pelvis, ECG, smart capillaroscopy, MRT, MRA, which provide with obtaining the integral picture of the cause-result connections between functional systems of blood circulation (macro-, regional and microvascular) and respiratory.
2. Optimum parameters’ selection of the cardiovascular, respiratory and excretory systems’ functioning for providing the stability of neurodynamic processes with the formation of a tendency to increasing of the amplitude-frequency indexes of the neurodynamic activity.
3. Formation of optimum boundary parameters of the cardiovascular, respiratory and neurodynamic systems’ activity when performing neurorehabilitating loads in order to prevent critical deviations in the stable functioning of all systems in the organism.
4. Individual selection of neurorehabilitating programs for a certain patient using massage, kinesitherapy, biorythmcorrection, psychological and logopedic stimulating correction, aromatherapy depending on the analysis of the data obtained from the previous diagnostics of neuropsychological status, state of the articular- speech organs, muscular tonus and their ability to passive-active motions, ways of the organism’s reactions to external stimuli.
The instrumental monitoring during treatment of patients with apallic syndrome: USDG, EEG, smart optical capillaroscopy.
Despite of the present level of diagnostics doctors don’t know about feelings of the unconscious state and so far they don’t seek for their objective appraisal. Therefore, only positive treatment to any even the most serious patient can be the optimum solution of this bioethical problem. Any conversation with doctors, nurses and relatives about possible negative consequences should be held very carefully and in no circumstances in the presence of the patient. And all rules of deontology should be applied to the patient in the critical state.


Rancho Los Amigos Scale (D. Malkmus et al., 1980, USA) provides the insight of progressive restoration of brain functions via recovery and rehabilitation.
1. No response: a patient is in a state of deep sleep and doesn’t respond to any stimuli.
2. Generalized responses: a patient responds inconsistently and non purposefully to stimuli in a nonspecific manner. His reflexes are limited and the same, regarding the stimuli.
3. Localized response: patient’s responses are specific, but not synchronous, and are directly related to the stimuli presented. The process of turning head towards a sound or focusing of the sight on the present object is a complicated act of involving of some brain sections into the activity. The patient can follow simple commands without synchronization of the higher cortical functions and/or with certain delays.

4. Confused-agitated level: patient is in a heightened state of activity and severely confused, disorientated, unaware of present events. His behavior is often strange and inappropriate to his environment. He is unable to perform self-care. If not physically disabled, he may perform automatic motions such as sitting, reaching and walking as a part of his agitated state, but not necessarily as a purposeful motion. Some patients may have long-term persistent states of the automated aggression up to the physically weakest and the most non-protected relative (according to the behavior), as a rule to his own mother.
5. Confused- inappropriate, non-agitated level: a patient appears alert and responds to simple commands. But more complex commands require responses that are non purposeful and random. The patient may show agitation that relate more to external stimuli rather than internal confusion. The patient is very distractive and generally has complications in learning new information. He can manage self-care activity with some assistance. His operative memory is very worse, long-term memory is almost absent, or can be lost for the last 3-5-10-20 years of his life, which used to be before coma. The speech is often unclear, signs of motor-sensor aphasia, amnestic aphasia are possible, often echolalia are apparent, excessive concretization of expressions is possible when the logical thinking is absent.
6. Confused-appropriate level: a patient shows goal-directed behavior but relies on hints for direction. He manages to renew old skills such as activity of daily living, but new information creates problems for his memory. He has a beginning of awareness of himself and others. We can say only about the performed activity with the real absence of the conducted activity (the patient says that he goes to work, manages the enterprise, pays wages in time etc. although his attendance the job is limited only by sitting in the office, recognition of belongings, documents). Another patient was resentful against her mother for the reproof regarding some stereotype actions in a dressing-room, which she didn’t make (she didn’t sew water). However the patient insisted that she had done this, but actually the action had not been performed.


7. Automatic – appropriate level: a patient automatically manages daily activity but it is robot-like behavior with minimal confusion. He has superficial recalls of activities and non-critical awareness of his condition. He requires at least minimal treatment, assistance in his problems’ solving and in planning the further activity.
8. Purposeful-appropriate level: a patient is alert and oriented, is able to recall and integrate the past and recent events. He can learn new activities and go on to study the house and master new living skills, but has lack in stress tolerance, social, emotional, and intellectual overloads.
We have assigned 4 basic stages in rehabilitation of patients regardless the etiological factor:
А. Planning of total deregulations in functional systems
(1st level of Rancho Los Amigos Scale);
B. A stage of crystallization of residual (preserved) functions of the central nervous system (2nd -3rd level of Rancho Los Amigos Scale). Corresponds with a stage of akinetic mutism;
C. A stage of stimulation and development of neuroplastic ability of the defective functional system of the brain and spinal cord, which corresponds with a stage of the minimal consciousness (3rd-5th level of Rancho Los Amigos Scale);
D. A stage of formation of final motor compensation and restoration of age mental activity of the personality (6-8th level of Rancho Los Amigos Scale) corresponds with a stage of having the high consciousness.

